Forms & Applications
Download. Print. Repeat as Needed.On this page you will find some of MedBen’s most commonly used forms that you can download, print and sign. If you have any questions about using and completing these forms, please contact MedBen Customer Service at 800-686-8425 or medben@medben.com. Plan Administrators are welcome to contact their Account Representative.
In addition to the forms found below, MedBen also offers customer-specific resources for Employers, Members, Brokers and Providers on their respective site pages.
Medical and Pharmacy
Prescription Prior Authorization Request Form – Use for all pharmacy benefits managers except Ventegra (check your ID card to find your PBM).
Prescription Prior Authorization Request Form – Use for Ventegra only (check your ID card to find your PBM).
Covid Home Test Paper Claim Form (Ventegra) – Use this form to request reimbursement from Ventegra when you have purchased a Covid Home Test Kit at retail cost (check your ID card to find your PBM).
Dental
Dental Employee Application – Apply or make coverage changes.
Dental AND Vision Employee Application – Apply for dental and/or vision coverage or make coverage changes.
Vision
Vision Employee Application – Apply or make coverage changes.
Vision AND Dental Employee Application – Apply for dental and/or vision coverage or make coverage changes.
FSA
Employee’s Guide to Flexible Spending Accounts (with Debit Card) – Overview/FAQ of MedBen FSAs for plan participants who use MedBen debit cards.
Employee’s Guide to Flexible Spending Accounts (No Debit Card) – Overview/FAQ of MedBen FSAs for plan participants who don’t use MedBen debit cards.
FSA Mileage Reimbursement Form – For claiming under your Health FSA the mileage used to obtain qualified medical services from a physician, hospital or facility to prevent or alleviate a physical disease, defect or illness.
Debit Card Substantiation Form – Substantiate purchases made with your MedBen Debit Card.
Orthodontia Services Reimbursement Request Form – An orthodontist (or authorized bookkeeper) can use this form to request reimbursement for services.
Request for Debit Card – Request a debit card for your dependent or replace a lost or stolen card.
Health Care FSA Examples of Qualified Medical Expenses – Examples of services and medical products that can be purchased with FSA funds.
Limited Purpose Health Care FSA Examples of Qualified Medical Expenses – Examples of dental and vision services and products that can be purchased with limited purpose FSA funds.
Sample Letter of Medical Necessity – If a Letter of Medical Necessity is required from your provider to receive reimbursement from your FSA, this sample letter can be used for that purpose. Simply print out/save and give to your doctor.
FSA Reimbursement Request Form – Used when requesting reimbursement from a Health FSA plan, Limited Purpose FSA plan and/or Dependent Care reimbursement plan.
HRA
COBRA
HRA Reimbursement Request Form – Request reimbursement from your HRA account. NOTE: This form is generic and may not be specifically based on your employer’s HRA plan design.
HIPAA
Access to Personal Information Request Form – Request access to copy or inspect personal health information held by MedBen.
Request to Restrict Uses and Disclosures of Protected Health Information – Request restrictions of the use or disclosure of personal health information held by MedBen.
Request for Personal Identification Number – Request MedBen to provide a Personal Identification Number (PID) for a plan member.
PHI Disclosure Accounting Request Form – Request an accounting of disclosures made by MedBen of your health and medical information.
Confidential Communication Request Form – Request alternate means of communication with MedBen.
PHI Amendment Request Form – Request MedBen to make corrections or amendments to your protected health information.
Notification and Authorization of Personal Representative Form – Designate an individual as your personal representative for purposes of coverage under selected health plan(s).
Authorization Form for Uses and Disclosures of Insured Information – Authorize the use or disclosure of your individually identifiable and/or personal health information.
Privacy Complaint Form – Register a complaint if you believe anyone at MedBen has inappropriately used or disclosed protected health information.
Other
Disability Claim Form – Plan members can submit a claim for long-term or short-term disability benefits.
Transportation Reimbursement Form – Plan members can request reimbursement from their transportation compensation account.
Notice of Appeal/Designation of Authorization Form – Plan members wishing to file a formal appeal of a disputed claim should use this form. They can also designate another entity to file an appeal on their behalf. (Please print and sign form before sending.)
Death Claim Form (Life Insurance Claim) – Please contact MedBen Customer Service (800-686-8425 or medben@medben.com) to obtain a death claim form. Employers must complete and return this form (accompanied by a certified copy of the death certificate) in order for designated beneficiary to receive life insurance benefits.
Self-funding Saves. MedBen Delivers.
Download the MedBen Client Report
Please register to download the Client Report. Thanks!
Benchmarking
MedBen Analytics' benchmarking capabilities enable you to compare your data against state and national norms and/or specific industries. You can narrow your benchmarks by plan type, number of lives and other metrics to get a true measure of how your plan stacks up.
Your benchmarking choice is immediately reflected on the dashboard content.

Straight RBP
Providers receive fair reimbursement by using Medicare pricing as the primary source of repricing. And because your plan no longer has a PPO, your plan members can go anywhere they choose for medical care.
Pharmacy Cost Plus Pricing
RBP for your prescription drugs.
Layered RBP
Target high-cost medical treatments, such as kidney dialysis.
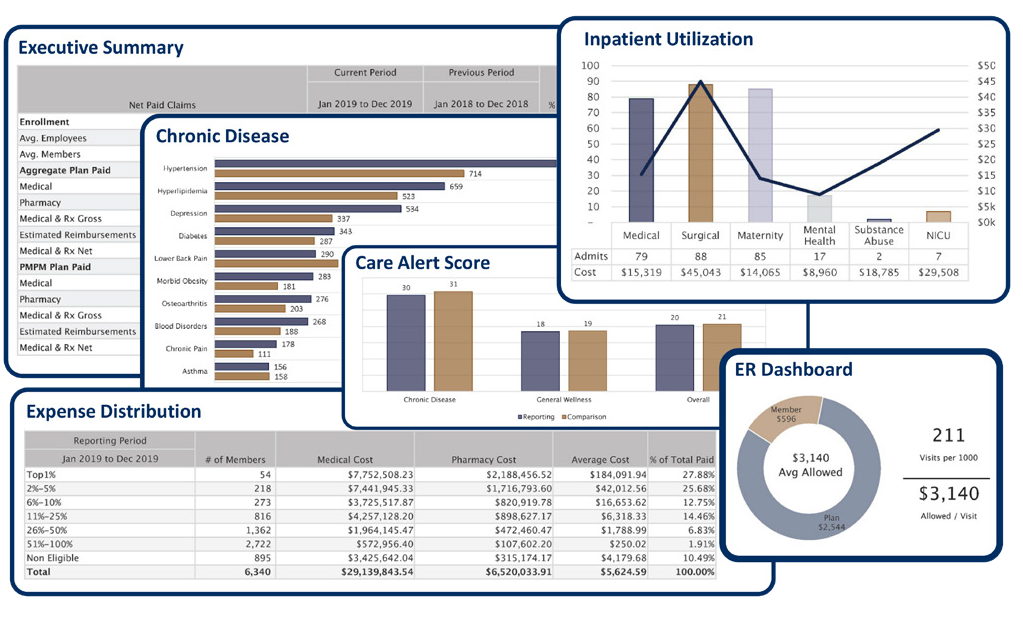
An Extensive Reporting Library
Once you've chosen your population, reporting period and benchmark preferences, just sit back and watch MedBen Analytics go to work for you. Dozens of charts, graphs and tables, instantly generated. Our financial, clinical, risk and savings reports show you what is working with your plan while highlighting areas of potential improvement.
![]() FSA Store is the largest online marketplace for guaranteed FSA-eligible products, helping flexible spending account holders manage and use their FSAs and save on more than 4,000 health items using tax-free money. You can pay for purchases using your MedBen FSA debit card so they are automatically noted on your account balance.
FSA Store is the largest online marketplace for guaranteed FSA-eligible products, helping flexible spending account holders manage and use their FSAs and save on more than 4,000 health items using tax-free money. You can pay for purchases using your MedBen FSA debit card so they are automatically noted on your account balance.
Use these convenient links for finding FSA-eligible products and calculating your FSA tax savings. FSA members can check their current account balances by visiting MedBen Access or downloading our mobile app from the Apple App Store or Google Play (search for "MedBen").

{kind=link}
Use this secure 24/7 service portal to access claims and benefits information. MedBen Access enables you to:
- Check claims status
- Review benefit coverages
- Download explanations of benefits (EOBs)
- See deductibles, out-of-pocket costs and calendar maximums
- Look up drug information, compare local pharmacy prices and check availability of lower-cost equivalents
- Review FSA and HRA activity and balances
- Check wellness exam and screenings compliance (for WellLiving members)
If you need assistance logging in to MedBen Access or using its features, please contact MedBen Customer Service at 800-686-8425.
MedBen Access is also available as a mobile app with the same great features! Download it from the Apple App Store or Google Play (search for "MedBen").
Download the MedBen Client Report
Please register to download the Client Report. Thanks!
Frequently Asked Questions about using the debit card (PDF).
Download a list of participating pharmacies, discount stores and supermarkets that can identify FSA-eligible items at checkout using an Inventory Information Approval System (IIAS).
Download a list of participating pharmacies, discount stores and supermarkets that do not use IIAS, but 90% of whose sales come from medical care items (thus making them FSA-eligible).
Medical Solutions.
MedBen will work with your clients to find the best solution to meet specific employee population needs. Increasingly, organizations are going outside the PPO box and turning to direct-to-employer contracting, reference-based pricing, and other alternative reimbursement strategies with set pricing that makes it easier to predict expenses. And their members can visit the doctors they prefer and still realize lower out-of-pocket costs.

Pharmacy Solutions.
MedBen will work with your clients to find the best solution to meet specific employee population needs. Increasingly, organizations are going outside the PPO box and turning to direct-to-employer contracting, reference-based pricing, and other alternative reimbursement strategies with set pricing that makes it easier to predict expenses. And their members can visit the doctors they prefer and still realize lower out-of-pocket costs.
Medical Solutions.
MedBen will work with your clients to find the best solution to meet specific employee population needs. Increasingly, organizations are going outside the PPO box and turning to direct-to-employer contracting, reference-based pricing, and other alternative reimbursement strategies with set pricing that makes it easier to predict expenses. And their members can visit the doctors they prefer and still realize lower out-of-pocket costs.
Pharmacy Solutions.
MedBen Rx follows a simple philosophy: The client's money belongs to the client. Our pharmacy solutions are designed to get members the right drug at the lowest cost, with total transparency to the employer. These include:
- Pricing solutions that ensure clients pay just what the pharmacies pay.
- Appropriateness solutions to find the most effective drugs at the best cost.
- Access solutions that give members new ways to lower their drug cost.


Direct-to-Employer Contracting
Many MedBen clients blend their RBP plan with direct-to-employer (DTE) contracts, which promote the use of quality care through local providers. In exchange for encouraging members to visit contracted facilities, providers bill the plan at mutually agreed-upon rates.
MedBen has been facilitating DTE contracting for over a decade with doctors and hospitals across the Midwest, and we continue to gain access to more exclusive DTE contracting. This strategy ensures that when members utilize area providers, they receive the best pricing options available.